Creating Civil Commitment Chaos
Minnesota taxpayers wasted $118,000,000 in 2019 on the Minnesota Sex Offender Program (MSOP) and according to Eric Janus, Professor of Law at the Mitchell Hamline School of Law, "…over 400 human beings are being held unconstitutionally... an intentional design feature of MSOP…”1 MSOP is already a waste of money considering that "Convicted sex offenders have among the lowest rates of same-crime recidivism of any category of offender..."2 But if what Professor Janus says is true, then MSOP might be guilty of fraud also We do not know what "design feature" Professor Janus is referring to specifically. However, we do know that health care fraud is common in the US Many psychiatrists and psychologists are disciplined or prosecuted each year for healthcare fraud In fact, in one 16-month period, 78 mental health workers in the US alone were convicted of fraud related activities; 30 convictions resulted in prison sentences totaling 72 years, and fines and restitution of more than $27 million3. We also know that the administrators of the MSOP have implemented a confusing treatment process and they warehouse detainees they know are not mentally ill.
MSOP clients should not have to sift through legal jargon and political bureaucracy to understand the laws that govern their treatment However, we are compelled to try. In this article we are going to explain how MSOP circumvents the law to keep people committed, even if the person does not have a mental illness However, in their attempt to sidestep the law to hold as many human beings, for as long as possible, MSOP has turned a simple issue chaotic Be patient with us while we explain the MSOP scheme and attempt to shed light on how complex MSOP has become.
MSOP is licensed to provide treatment," subject to the standards of Chapter 245A and Minnesota Rules part 9515.3000 to 9515.3110.”4' Meaning, these are the standards MSOP is required to follow when they administer treatment to their clientele. However, there is a law in Minnesota that allows the DHS commissioner to depart from the rules that govern MSOP. This departure is called a "variance." A variance is like a waiver that allows the license holder to do something other than what the license would normally permit.5 In 2005 MSOP applied for a "permanent variance" (variance #4 6) to Minnesota Rule 9515.3030 subpart 2. The rule states, "A psychiatrist must evaluate each person within three working days after the person is admitted and reevaluate each person at least annually".7 A permanent variance is restricted to protect detainees from being negatively affected by these changes. For instance, a permanent variance, "…cannot compromise the qualifications of staff to provide services ". However, with variance #4, the one that alters 9515.3030 subpart 2, MSOP no longer has to allow psychiatrists to evaluate detainees. Instead, MSOP can use either a "licensed mental health professional" or a "licensed-eligible psychologist".8 Although variance #4 is "…compromising the qualifications of staff..." MSOP never gave a time limit for it and has renewed it repeatedly throughout the years. The variance has remained in effect since 2005.9
1. Karsjens v. Jesson: Brief of Law Professors as Amici Curiae in Support of Petition for Writ of Certiorari: p.12, 1st Paragraph This may be available online, ERIC S JANUS* Professor of Law MITCHELL HAMLINE SCHOOL OF LAW 875 Summit Avenue St Paul, MN 55105 Telephone (651) 290-6345 Email cricjanus@mitcheilhamline.edu
2. David Feige When Junk Science About Sex Offenders Infects The Supreme Court" The New York Times, 12 Sept 2017 Szasz, Thomas "Psychiatric Abuse Facts" Citizens Commission on Human Rights, contact@cchr.org
4. Exhibit A Minnesota Department of Health license Read under Terms of License" [pg. 5] to identify what MSOP is licensed to do.
5. Exhibit B Minn. Stat § 245A.04 Sub 9 Variances Pay close attention to the underlined section in this exhibit
6. Exhibit C Variance Request Application At the top right corner of the first page [p 8] written in pen it says "Variance #3, (3030-2)" This is not accurate It should say "Variance #4, (3030-2)" If you look at the next page [p 10] on the third line of the text it says, "Rule Part (enter complete number) 9515 3030 Subpart 2" Also, In Exhibit D Summary of All Variances, this is listed as "Variance #4" [p 21]
7. STATE HOSPITAL ADMINISTRATION 9515 3000, MINNESOTA SEXUAL PSYCHOPATHIC PERSONALITY TREATMENT CENTER 9515 3030 EVALUATION, ASSESSMENT, AND TREATMENT PLANNING Subp 2 Psychiatric evaluation
8. Exhibit D Summary of All Variances See Variance #4 [Pg. 21] The original rule that MSOP is licensed for is in the left column The new rule allowed by the variance is in the right column Notice how the variance changes the qualifications of staff.
9. Exhibit C: Variance Request Application: On the second page [p. 10] you will see that the space for "Length of Time is empty.
Not all MSOP detainees need treatment. Minnesota Rule 95 15.3030 subpart 2 is governed by a particular Minnesota law, and must reflect the intent of that law. The law that governs the rule states, in relevant part, "The commissioner shall establish an evaluation process to measure outcomes and behavioral changes as a result of treatment compared with incarceration without treatment, to determine the value, if any, of treatment in protecting the public."10 This law tells us that it is not necessary to provide treatment to all detainees. Some will need it. Some will not. In addition, the law that governs a detainee's discharge from MSOP says if a detainee "...is no longer in need of treatment and supervision..."11 he must be released. However, without each detainee getting evaluated by a psychiatrist, there is no way to know who no longer needs treatment.
Variance #4 allows a "licensed mental health professional" or a "licensed-eligible psychologist" to do assessments. But neither is a psychiatrist, who is able to identify mental illness. The Minnesota Judiciary has consistently ruled that a person must have a "mental illness" to be committed to MSOP. A "Person who is mentally ill" is defined by Minnesota law as ". . . any person who has an organic disorder of the brain or a " attempt or threat to physically substantial psychiatric disorder..." which is often demonstrated by, “...a recent I? harm self or others..."12 In addition, the DSM-5 -- used by psychiatrists to diagnose mental illness - requires that an individual display a "current presentation" of mental illness for the detainee to get branded with a diagnosis. For sexual disorders, "current presentation" is within 6 months.13 In other words, if the detainee has not shown any signs of mental illness as described by the DSM-5, then he is in remission, and must be released.
Mental illness is a medical issue in the same way the illness of cancer is a medical issue. Do you go to a medical doctor to get chemotherapy for a cancer you used to have? No. You could only get chemo if you currently have cancer. In this way, medical illness is no different than mental illness. For someone to get civilly committed in Minnesota, a court has to find that the person is "mentally ill." According to Minnesota law, these individuals must go to a facility that, "...is consistent with the persons treatment needs..."14 So what kind of treatment does the detainee need? Well, they clearly need a type of treatment that addresses their current and recent behaviors. Therefore, an evaluation by a psychiatrist is in order. The reason is simple: a psychologist looks at past behaviors to conclude whether or not commitment is necessary. But a psychiatrist looks at recent behaviors to determine whether the detainee must be released. Therefore, the kind of treatment that would be "...consistent with the persons treatment needs..." would be a treatment provided by a psychiatrist. A "licensed mental health professional" or a "licensed-eligible psychologist" cannot provide adequate treatment to the MSOP client.
What was originally a straight forward rule is now two pages of confusion. The qualifications of staff were compromised by Variance #4 which substituted a psychiatrist for multiple clinical staff. Now, if the detainee is thought to have a mental illness, his case may be addressed by one of 11 different clinical staff, each with a different set of credentials. None of these staff persons are psychiatrists. If a psychiatrist does ever get involved with a detainee’s case, it could take up to 19 days after admission for the psychiatrist just to review the detainee's record, if they ever do at all.15 When MSOP Replaced the psychiatrist, they settled for a "licensed mental health professional" or a "licensed-eligible psychologist." This change made it impossible for
9. Exhibit C: Variance Request Application: On the second page [p. 101 you will see that the space for "Length of Time Requested for Variance" is empty.
10. Exhibit E: Minn. Stat. § 24613.04 RULES; EVALUATION: Pay close attention to the underlined section in this exhibit.
11. Exhibit F: Minn. Stat. §. 253D.31 DISCHARGE: Pay close attention to the underlined section in this exhibit.
12. Exhibit G: Minn. Stat. § 25313.02 Subd. 13 (a). Person who is mentally ill: Pay close attention to the underlined section in this exhibit.
13. Exhibit H: DSM 2nd Paragraph: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, American Psychiatric Publishing, Copyright 02013. p. 22. Also see pp. 685 —705 of the DSM. Not shown here.
14. Exhibit I: Minn. Stat. § 253D.07 Subd. 3: Pay close attention to the underlined section in this exhibit.
15. Exhibit D: Summary of All Variances: The original rule that MSOP is licensed for is in the left column. The new rule allowed by the variance is in the right column. Notice how the variance changes the qualifications of staff.
detainees to receive the type of quality treatment they need A psychologist is trained to look at past issues and behaviors —the same issues and behaviors used to determine the detainee's initial commitment - and use them to consider continued commitment The result hundreds of Minnesotans remain unlawfully detained because it is impossible to treat the unique clientele of MSOP with a treatment model that does not abide by the rules of the license.
Many of the laws used to govern MSOP are the same laws used to govern hospitals in Minnesota However, Clinical Director of MSOP, Ms. Jannine Hebert, gave testimony on March 5, 2015 before, The Honorable Donovan Frank, and explained that the MSOP has not been a hospital since at least 2008. In fact, according to Ms. Hebert, MSOP is a "treatment program" that deals with folks who are "not sick".16 In addition to Ms. Herbert's statement, the variance request for Variance #4, explicitly confesses, "The vast majority of patients committed to the Minnesota Sex Offender Program do not experience symptoms of mental illness that requires psychiatric treatment.17 This is a problem, because one cannot receive medical care and attention at a facility that does not provide medical services. More importantly, the law requires that in order to lock someone up in a mental institution, they need to have a mental illness.
On December 11, 2019 Ms. Johnston, Executive Director of MSOP, held a forum for detainees to ask her questions. She told detainees at MSOP that she had requested funding from the Minnesota legislature to expand the MSOP program. She was then asked by a detainee if she would be willing to get a psychiatrist to evaluate the entire MSOP population, potentially finding hundreds of detainees ready for discharge. She said it is "too expensive" and "out of [her] control" to authorize such evaluations. Another detainee then told her that if she were to ask the DHS commissioner to expire the variance, the commissioner likely would. The law would then require Ms. Johnston to hire a licensed psychiatrist to evaluate the MSOP detainees and the legislature would certainly fund the evaluations, especially if doing so is in the interest of the law. She said that she did not know anything about the variances, even though she gave testimony on March 2, 2015, before The Honorable Donovan W Frank, about them18, and she signed the paperwork.19
In addition to the limitations of a variance that we have already mentioned, a variance also" cannot affect the health or safety of the patients…". Perhaps one or two variances would not affect the health and safety of detainees. But the culmination of them all have kept detainees indefinitely detained without providing treatment to them MSOP currently has at least 15 variances that alter Minnesota Rules 9515 3000 —9515.3110, the rules for which MSOP is licensed to provide treatment. Using variances, MSOP dramatically altered the entire treatment process of MSOP, and moved the facility away from a Medical Model. Therefore, MSOP cannot administer adequate treatment services to "ill" people. The administrators of the Minnesota Sex Offender Program (MSOP) have implemented a confusing treatment process in order to warehouse detainees they know are not mentally ill Expiring the variances - especially the ones that are clearly illegal - would at least simplify the issue enough to consider the next step toward MSOP Reform.
Join the petition and call your local legislators to tell them to expire the MSOP variances.
16. Exhibit J: Karsjens v. Jesson Vol. XVIII: dated March 5, 2015, pp. 3957, 3958 (cover page) 4001, 4002 (Hebert's Testimony), Case No I l-CV-3659 (DWF/JJK)
17. Exhibit C Variance Request Application [p 12]
18. Exhibit K Karsjens v Jesson Vol XV dated March 2, 2015, pp. 3198, 3199 (cover page), 3336 (Johnston's testimony about the variances), Case No 1 I-CV-3659 (DWF/JJK)
19. Exhibit D: Summary of All Variances: [ p. 53].
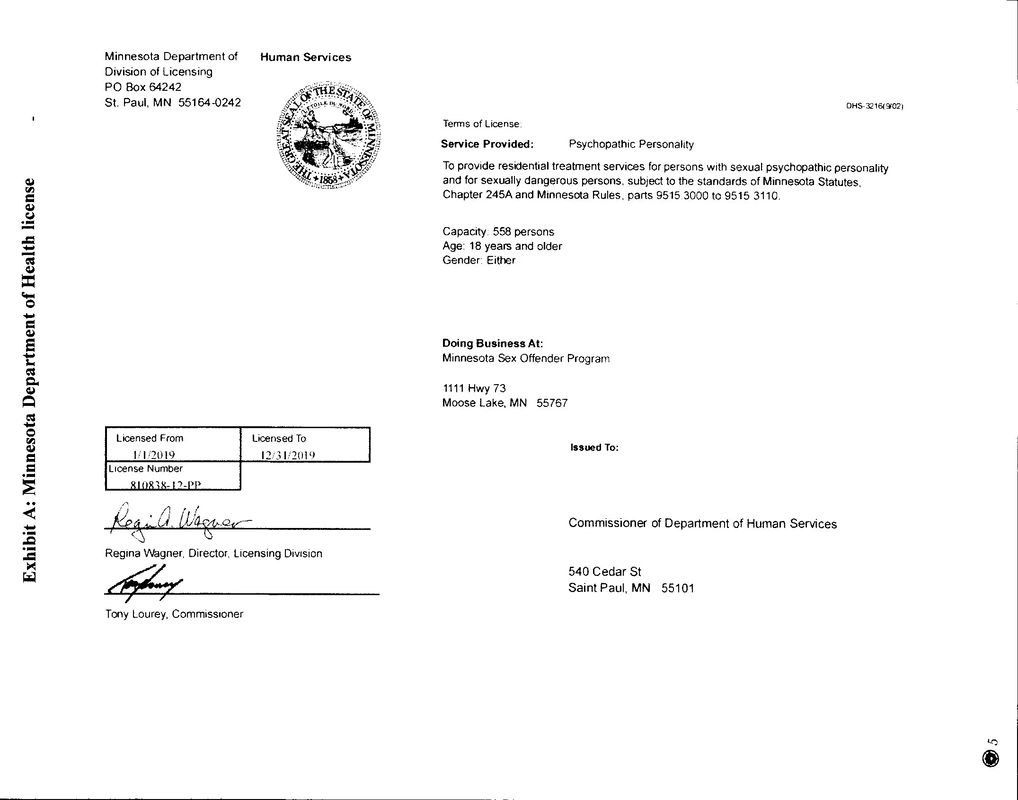
Exhibit B: Minn. Stat.§ 245A.04 Subd. 9 Variances.
- (a)
The commissioner may grant variances to rules that do not affect the health or safety of persons in a
licensed program if the following conditions are met:
- (1) The variance must be requested by an applicant or license holder on a form and m a manner
prescribed by the commissioner
- (2) the request for a variance must include the reasons that the applicant or license holder cannot comply
with a requirement as stated in the rule and the alternative equivalent measures that the applicant or license
holder will follow to comply with the intent of the rule; and
- (3) the request must state the period of time for which the variance is requested.
The commissioner may grant a permanent variance when conditions under which the variance is requested
do not affect the health or safety of persons being served by the licensed program, nor compromise the
qualifications of staff to provide services. The permanent variance shall expire as soon as the conditions that
warranted the variance are modified in any way. Any applicant or license holder must inform the commissioner
of any changes or modifications that have occurred in the conditions that warranted the permanent variance.
Failure to advise the commissioner shall result in revocation of the permanent variance and may be cause for
other sanctions under sections 245A.06 and 245A.07.
The commissioners decision to grant or deny a variance request is final and not subject to appeal under the
provisions of chapter 14.
- (b)
The commissioner shall consider variances for child care center staff qualification requirements under
Minnesota Rules, parts 9503.0032 and 9503.0033, that do not affect the health and safety of children served by
the center. A variance request must be submitted to the commissioner in accordance with paragraph (a) and
must include a plan for the staff person to gain additional experience, education, or training, as requested by the
commissioner. When reviewing a variance request under this section, the commissioner shall consider the staff
persons level of professional development, including but not limited to steps completed on the Minnesota career
lattice.
The commissioner may grant a permanent variance when conditions under which the variance is requested do not affect the health or safety of persons being served by the licensed program, nor compromise the qualifications of staff to provide services. The permanent variance shall expire as soon as the conditions that warranted the variance are modified in any way. Any applicant or license holder must inform the commissioner of any changes or modifications that have occurred in the conditions that warranted the permanent variance. Failure to advise the commissioner shall result in revocation of the permanent variance and may be cause for other sanctions under sections 245A.06 and 245A.07.
The commissioners decision to grant or deny a variance request is final and not subject to appeal under the provisions of chapter 14.
Exhibit D: VARIANCE to the RULE 26 LICENSE
for the MINNESOTA SEX OFFENDER PROGRAM (MSOP)
February 1, 2014
- The Rule 26 requirements are listed in the Rule Part column. The text highlighted in gray identifies the requirement(s) for which the license holder requested a variance. Text that is not highlighted in gray is not affected by the variance.
- The license holder must comply with the licensing requirements in Rule 26 for which variances were not requested and must comply with the variance requirements in the right column as alternative equivalent measures to meet the intent of the rule requirement for which a variance is approved.
| RULE PART (RULE 26) REQUIREMENTS | VARIANCE REQUIREMENTS | 9515.3000 DEFINITIONS |
|---|---|
Subp. 2. Commissioner"Commissioner" means the commissioner of the Minnesota Department of Human Services or the commissioner's designated representative. | |
Subp. 3. Department"Department' means the Minnesota Department of Human Services. |
|
Subp. 4. Minnesota Sexual Psychopathic Personality Treatment Center"Minnesota Sexual Psychopathic Personality Treatment Center means the secure facility established at Moose Lake by Minnesota Statutes, |
Variance #1 to Minnesota Rules, part 9515.3000, subpart 4.A. In accordance with Minnesota Statutes, section 246B, MSOP will admit only clients on a court-hold order, pending commitment, courts as sexual psychopathic personalities, or sexually dangerous persons to committed by the MSOP program. NOTE: As amended, Minnesota Statutes, 24613.02 no longer permits clients to be admitted solely based on the consent of the commissioner. B. A license to each facility will be issued, but MSOP may operate as one program at two separate locations, provided the license holder operates under ones of policies and procedures and under one administration. NOTE: This variance does not affect the requirements in Minnesota Statutes, chapter 245C, including those related to the person(s) designated to receive sensitive background study information and how set asides of disqualifications are managed. This includes but is not limited to the requirements in Minnesota Statutes, sections 245C.07 and 245C. I 4. C. The name of the program will be that given in Minnesota Statutes, section 246B.02, Minnesota Sex Offender Program (MSOP). |
| Subp. 5. Person or person in treatment. "Person" or "person in treatment" means a person committed to the Minnesota Sexual Psychopathic Personality Treatment Center or admitted there with the consent of the commissioner as provided in Minnesota Statutes, section 246B.02. | |
| Subp. 6. Sexually dangerous person. "Sexually dangerous person" has the meaning given in Minnesota Statutes, section 253B.Q2, subdivision 18b. | |
| Subp. 7. Sexual psychopathic personality. "Sexual psychopathic personality" has the meaning given in Minnesota Statutes, section 2538.02, subdivision 18a. |
|
| Subp. 8. Treatment staff. "Treatment staff" means staff members of the Minnesota Sexual Psychopathic Personality Treatment Center who are responsible for arranging, evaluating, planning, coordinating, or providing the programming and services required in part 9515.3040, subpart 1. |
|
| Subp. 9. Treatment support staff. "Treatment support staff" means staff members of the Minnesota Sexual Psychopathic Personality Treatment Center whose primary responsibility is to maintain a secure and orderly environment supportive of treatment by performing such duties as escorting persons, observing persons' behavior, and directing group activities on the unit. |
|
| 9515.3010 PURPOSE AND APPLICABILITY. Parts 9515.3000 to 9515.3110 apply only to residential treatment programs operated by the commissioner primarily for persons committed as sexual psychopathic personalities or as sexually dangerous or admitted with the commissioner's consent. The purpose of parts 9515.3000 to 9515.3 I 10 is to govern the operation, maintenance, and licensure of these department-administered treatment program. As of October 30, 1995, the Minnesota Sexual Psychopathic Personality Treatment Center at Moose Lake is the only such treatment program |
Variance #2 to Minnesota Rules, part 95 I 5.30 l 0. The same requirements set forth under variance # I to Minnesota Rules, part 9515.3000, subpart 4, are required of the license holder to meet the variance to Minnesota Rules, part 9515.3010. |
| 9515.3020 PROGRAM ADMISSION CRITERIA. Except when admitted with the commissioner's consent as provided in Minnesota Statutes, section 246B.02, persons admitted to a treatment program licensed under parts 9515.3000 to 9515.3110 must meet one of the criteria in items A to C. A. A court hold order is in effect under a petition for the person's commitment as a sexual psychopathic personality or sexually dangerous person. B. A warrant of commitment has been issued for the person as a sexual psychopathic personality or sexually dangerous person pursuant to Minnesota Statutes, chapter 253B. C. Final commitment action committing the person as a sexual psychopathic personality or sexually dangerous person has been taken under Minnesota Statutes, chapter 253B. | |
| 9515.3030 EVALUATION, ASSESSMENT, AND TREATMENT
PLANNING. Subpart 1. Multidisciplinary assessment. The license holder must assess each person entering the treatment program within ten days after admission to determine the person's need for medical care, nursing services, psychological services, social services, chemical dependency treatment, education and vocational training, and recreation and leisure activities. After the initial assessment, the license holder must update assessments on all persons at least annually. |
Variance #3 to Minnesota Rules, part 9515.3030, subpart 1. A. Within ten (10) calendar days of the client's admission, treatment staff will conduct admission assessments to identify the client's needs in the following areas: medical care; mental health; chemical dependency; and educational, therapeutic recreation, and vocational services. B. Treatment staff will interview the client individually to complete the admission assessments. The admission assessments will be completed in accordance with the license holder's policies and procedures and must include sufficient information to inform the client's individual treatment plan (ITP). C. All clients on the admissions unit, regardless of their commitment status, will be offered an opportunity to participate in sexual offender programming. For clients who are admitted on or after December 7, 2010, the opportunity to participate in sexual offender programming must be made within 14 calendar days of their admission. D. Clients under final commitment to the program under the Civil Commitment Act must be offered the opportunity to participate in a sexual offender assessment within 14 days of their final commitment. The offer and the client's response must be documented in the client record. For purposes of this item, "final commitment" means an order by a district court committing the individual as SOP or SPP or both. E. The sexual offender assessment must include an interview with the client. The results of the assessment will be incorporated into the client's ITP within 14 days. The sexual offender assessment must be completed within 30 days from the date the assessment was initiated. F. For clients who elect to participate in a sexual offender assessment, it must be initiated within 14 days of the client's election to participate in the sexual offender assessment. G. Sexual offender programming that occurs on the admissions unit or prior to a sexual offender assessment shall include educational, therapeutic recreation, and vocational services and a minimum of one therapeutic group per week pertinent to sexual offender treatment. H. The clients' admission assessments shall be updated annually. Annually has the meaning given it in Minnesota Statutes, section 245A.02, subdivision 2b. For clients admitted prior to May I, 20 l 0, their last assessments shall be updated annually. Annually has the meaning given it in Minnesota Statutes, section 245A.02, subdivision 2b. The following assessments must be updated: medical care, if needed; mental health; and educational, therapeutic recreation, and vocational services. The update of the assessment means staff from the multidisciplinary team review the client's treatment progress. This review shall consider the client's reaction to treatment goals. The client's ITP is updated as appropriate based on feedback from the client and the multidisciplinary team about the client's treatment progress. The revisions to the ITP will consider feedback from the client and multidisciplinary team. I. For clients who have completed a sexual offender assessment and are participating in sexual offender treatment, the assessment must be updated as described in paragraph H of this section as part of the annual meeting and the results of the update must be incorporated into the treatment plan. J. The license holder must maintain a policy and procedure specific to the admission assessments (completed within IO days of admissions) and the assessment updates (completed annually). Annually has the meaning given it in Minnesota Statutes, section 245A.02, subdivision 2b. The policy and procedures and related tools must be dated and approved by the MSOP Executive Director, or designee. |
| Subp. 2. Psychiatric evaluation.
A psychiatrist must evaluate each person within three working days after the person is admitted and revaluate each person at least annually. |
Variance #4 to Minnesota Rules, part 9515.3030, subpart 2. A. A licensed mental health professional, as defined in Minnesota Statute, section 245.462, subdivision 18, or license-eligible psychologist, must conduct an initial evaluation within three business days after the client's admission to determine whether the client has mental health needs. The initial screening must also determine whether the client has been prescribed any psychotropic medications and whether the client has mental health needs. B. When the licensed mental health professional's or license-eligible psychologist's initial screening under paragraph A of this section indicates a that psychotropic medication may be indicated for the client, a referral must be immediately made to a physician, advance practice registered nurse, or physician's assistant, who must evaluate the client within six business days from the date of the referral. C. When a physician (who is not a psychiatrist) or an advance practice nurse (APRN) or a physician's assistant (PA) prescribes or monitors the client's use of psychotropic medications, a psychiatrist must review new, modified, and discontinued prescriptions for psychotropic medications. The review must occur within IO days of the order or the change to the order and be documented. The documentation must be client specific. NOTE: Psychotropic medication means a medication prescribed to treat mental illness and associated behaviors or to control or alter behavior. The major classes of psychotropic medication are antipsychotic or neuroleptic, antidepressant, antianxiety, antimania, stimulant, and sedative or hypnotic. Other miscellaneous classes of medication are considered to be psychotropic medication when they are specifically prescribed to treat a mental illness or to alter behavior based on a client's diagnosis. See Minnesota Rules, part 2960.0020, subpart 59. D. Clients who are prescribed psychotropic medications must be seen by a psychiatrist at least every 12 months, including when the prescription was discontinued since the last annual visit. The meeting must be face-to-face or may be conducted via telemedicine provided that it is a private, visual, real-time interaction between the psychiatrist and client. If the client refuses to meet with the psychiatrist, the refusal and the reason for the refusal (if given) must be documented in the client's record. E. The screening (under paragraph A of this section) must be documented in the client record and all mental health needs, including those related to psychotropic medications must be integrated into the client's ITP. F. The license holder must maintain a policy and procedure that includes the screening tool to be used to conduct the initial screening. The policy and procedures and related tools must be dated and approved by the MSOP Executive Director, or designee.
|
| Subp. 3. Follow-up to psychiatric evaluation. Specific mental health interventions indicated in addition to the usual sex offender treatment program must be prescribed and monitored by a psychiatrist. These interventions must be integrated into the treatment plan. |
Variance #5 to Minnesota Rules, part 9515.3030, subpart 3. B. When a client requests psychotropic medication or to be seen by a psychiatrist, an individual who meets the requirements in variance number 4, paragraph C (variance to Minnesota Rules, part 9515.3030, subpart 2), namely, a physician, advance practice registered nurse, or a physician's assistant, or a licensed mental health professional (as defined in Minnesota Statute, section 245.462, subdivision 18), must meet with the client. As appropriate, the a physician, advance practice registered nurse, physician's assistant, licensed mental health professional, or license-eligible psychologist, will take steps to address the client's needs. In cases where the client, continues to request to see a psychiatrist, the physician, advance practice nurse, physician's assistant, or licensed medial health professional, will document the meeting with the client, and forward the necessary information to the psychiatrist. The psychiatrist will evaluate and determine whether it is appropriate for the client to be seen by a psychiatrist. C. When clients file grievances concerning the prescribing practices related to psychotropic medications, the review and response to the grievance will be conducted in accordance with Minnesota Statutes, section 245A.04, subdivision 1, paragraph (d), and must include consultation with a psychiatrist. D. Clients who are prescribed psychotropic medications shall have the option to receive psychotropic medication management from an individual who meets the requirements in variance number 4, paragraph C (variance to Minnesota Rules. part 9515.3030, subpart 2), namely, a physician, advance practice registered nurse, or physician's assistant. E. The license holder must assure that arrangements are made for the client to receive medication management services in a reasonable time frame. The license holder must assist the client as needed to assure that any follow-up appointments are arranged. F. All mental health needs, including those related to psychotropic medications must be addressed in the client's ITP. |
| Subp. 4. Individual treatment planning. Within 14 days after a person is admitted, a multidisciplinary team led by the program director or program director designee must develop and begin implementing a written treatment plan for the person. Based on the assessments and evaluation in subparts 1 and 2, the plan must identify the person's needs; determine the phase of treatment where it is most appropriate for the person to begin treatment; establish goals; assign staffing responsibility; and provide for at least quarterly review. At a minimum, the team must include the person, a psychologist, a social worker, a nurse, and a member of the treatment support staff. When psychiatric or medical treatment is required, a physician must also be included on the team. The case manager assigned by the county responsible for providing the person's social services must be notified of and given the opportunity to participate in all team meetings. Treatment staff who provide services identified in the treatment plan must also receive notice of team meetings and be given the opportunity to participate. |
Variance #6 to Minnesota Rules, part 9515.3030, subpart 4. A. For purposes of this variance, the program director means the executive clinical director or clinical director referenced throughout the variance. B. The multidisciplinary team will be led by the primary therapist assigned to the client. C. Within fourteen ( 14) calendar days of admission, the multidisciplinary team must develop a written ITP that addresses the needs identified through the admission assessments required in part 9515.3030, subpart I. At a minimum, this must include any needs related to: medical care; mental health; chemical dependency; and educational, therapeutic recreation, and vocational services. D. At a minimum, the multidisciplinary team must include the primary therapist, a licensed mental health professional as defined in Minnesota Statute, sections 245.462, subdivision 18, or license-eligible psychologist, a registered nurse, as appropriate, and a member of the treatment support staff. When medications or medical treatment is prescribed, a physician, advance practice registered nurse, or physician' s assistant must also provide input. The case manager, if assigned by the county, must be provided the opportunity to provide input to the multidisciplinary team. The client may provide input to the multidisciplinary team through the client's primary therapist. E. It must be documented in the client's individual file who was invited to participate in the client's treatment planning and who participated. F. Development of the initial ITP (within 14 days of admission) must include goals and interventions that are based on the admission assessments and the input from the multidisciplinary team concerning their admission assessments of the client in accordance with variance #3 of Minnesota Rules, part 9515.3030, subpart I. The ITP must also assign staff responsibilities related to implementation. G. For clients who elect to participate in sexual offender assessment and are under final commitment, the ITP will be updated in accordance with variance #3 to Minnesota Rules, art 9515.3030, sub rt 1, paragraphs H and I. H. The client must be provided a copy of the ITP within 30 days of admission (and any time it is revised). I. The client's treatment goals in the ITP must be reviewed quarterly and the client's progress toward reaching the goals identified for the previous quarter must be documented in the client's record. Quarterly is defined as within 90 calendar days of the previous multidisciplinary team meeting or previous quarterly review whichever is later. For people admitted to the program on or after May 1, 2010, the first quarterly review must be completed within 104 calendar days from the date of admission (i.e., within 90 calendar days of development of the initial ITP which must be completed within 14 calendar days of admission). For people admitted prior to May 1, 2010, the date that establishes the quarterly review cycle shall be the date of the client's last quarterly review or annual multidisciplinary meeting that occurs on or after February 1, 2010. J. At a minimum, the multidisciplinary team review completed quarterly must include input from a licensed mental health professional as defined in Minnesota Statute, sections 245.462, subdivision 18, or license-eligible psychologist, a registered nurse, as needed, and a member of the treatment support staff. The primary therapist coordinates the quarterly review and gathers the input needed (including reviewing documentation from all shifts by staff who are not members of the treatment team, but who have contact with the client on the living unit) to review the treatment goals in the ITP and update the ITP based on the input. When medications or medical treatment is prescribed, a physician, advance practice registered nurse, or physician's assistant must be provided the opportunity to provide input into the review. NOTE: Input means that members of the multidisciplinary team shall provide status updates, concerning their assigned responsibilities as related to the client's ITP, to the primary therapist prior to the client's quarterly review. K. As part of the therapeutic process. clients discuss their perception of their progress related to the quarterly review during groups with peers and their primary therapist. The client's input is documented by the primary therapist in the group notes. Clients wiII be provided a copy of their quarterly progress report. If the client's ITP is updated or revised the client shall be given a copy of their revised ITP within 30 days. Clients will also be given a copy of their ITP within 30 days of their annual progress review meeting. L. Annually a meeting will be held with the multidisciplinary team and the client. Annually has the meaning given it in Minnesota Statutes, section 245A.02, subdivision 2b. The meeting shall be coordinated by the primary therapist. At a minimum, the multidisciplinary team must include a licensed mental health professional as defined in Minnesota Statute, sections 245.462, subdivision 18, or license-eligible psychologist, a nurse, and a member of the treatment support staff. The nurse will represent issues related to medical treatment and medications. The meeting must provide the opportunity for all members of the multidisciplinary team to be present at the same time and be able to interact with the team. M. The annual meeting shall provide an opportunity for the members of the multidisciplinary team to provide status updates concerning their assigned responsibilities in the ITP. The primary therapist must gather input from staff working on the client's living unit, but who are not members of the multidisciplinary team. This input must include all shifts. The input of these staff must be summarized by the primary therapist at the annual meeting. Based on the information from the annual meeting and with input from the client, the ITP shall be revised. N. The revised ITP must identify the client's needs, treatment goals, interventions, and assigned staffs responsibility. The client shall receive a copy of the revised ITP within 30 days of the meeting and shall receive an annual treatment progress report. O. Clients must be provided the opportunity to participate in the annual meeting. It must be documented in the client record if the client elects not to participate in the meeting. P. The client's county case manager must be notified in writing and given an opportunity to participate in or provide input to the quarterly reviews and annual meetings. A copy of the notification must be placed in the client's individual record. Q. A list of the people who participated in each quarterly review and annual meeting and their title or for individuals who are not MSOP staff their relationship to the client must be documented in the client's record. |
| 9515.3040 TREATMENT PROGRAM SERVICES. Subpart 1. Scope of treatment program services. At a minimum, a license holder's program services and resources must include: A. specific programs that address sex offense behaviors and remediation, and include, as applicable, related topics such as deviant sexual arousal patterns, assaultive behavior, human sexuality, victimization issues, reoffense prevention, and interpersonal relationships; B. psychiatric, medical, dental, psychological, social, and advocacy services; C. educational programming; D. Assessment and treatment of chemical dependency and; E. vocational rehabilitation services; and F. leisure and recreational activities. The license holder must offer treatment in a form and structure consistent with a person's capacity to participate productively. |
Variance #7 to Minnesota Rules, part 9515.3040, subpart I, items A and D. A. The primary therapist assigned to the client is responsible to assure that the treatment program services are coordinated, provided, and accurately reflected in the ITP. B. For purpose of item A of Minnesota Rules, part 9515.3040, subpart I, "specific programs that address sex offense behaviors and remediation" is replaced with "sexual offender specific treatment." Sexual offender specific treatment means a comprehensive and integrated set of planned and organized therapeutic experiences and interventions that are intended to improve the prognosis, function, and/or outcome of clients to reduce the risk of sexual reoffense, or other sexually abusive and/or other aggressive behavior by assisting them to adjust to and deal more effectively with their life situations as defined in variance #3 to Minnesota Rules, part 9515.3030, subpart 1, items D, E, and F. C, As required in variance #3 to Minnesota Rules, part 9515.3030, subpart I, item A, treatment staff must conduct an assessment of the client's needs related to chemical dependency within IO days of admission. For purpose of paragraph D, in Minnesota Rules, part 9515.3040, subpart I, prior to being transitioned to community preparation services, the client must again be assessed for the need for chemical dependency treatment. If the assessment indicates the client is in need of chemical dependency treatment, the ITP must be amended and the client must be offered chemical dependency treatment. The license holder must provide or arrange for the provision of the chemical dependency treatment. |
| Subp. 2. Treatment-related policies and procedures. A license holder must develop and follow written policies and procedures that specify how the license holder will fulfill the responsibilities in items A to G. A. Meet data privacy laws and professional confidentiality standards, especially regarding the use and results of physiological examinations and the reporting of previously undetected criminal behavior which is disclosed by a person while in the program. B. Evaluate individual treatment outcomes and program outcomes, including indicators to be used and processes for program improvement. C. Prevent abuse and predation among program participants. D. Provide gender-specific treatment where appropriate. E. Respond to allegations of criminal acts committed by a person while in the program. F. Monitor for contraband. G. Provide a safe environment for staff, program participants, and visitors. |
Clarification: The license holder must have a grievance process that meets the requirements of Minnesota Statutes, section 245A.04, subdivision I, paragraph (d). The process must include a provision for appeal and review by the executive director. |
| 9515.3050 STAFFING REQUIREMENTS. Subpart 1. Program director. Each licensed facility must have at least one full-time program director who meets the requirements in part 9515 .3060. |
|
| Subp. 2. Number of staff; staffing patterns. The license holder must provide qualified treatment and treatment support staff in numbers sufficient to meet the license holder's responsibilities for evaluation and assessment, developing and implementing individualized treatment plans, providing a secure and orderly environment, and planning for discharge. The number and type of staff needed on a given unit at a given time are to be determined by the needs and characteristics of the persons on the unit in accordance with the ongoing staffing assessment required in subpart 3. |
|
| Subp. 3. Ongoing assessment and determination of necessary staffing levels. Staffing levels shall be assessed and determined as specified in items A to G. A. The license holder must perform assessments to determine the staffing levels necessary to meet the safety and treatment needs of program participants and the safety needs of staff The assessments must address staffing levels for both treatment and treatment support staff functions. B. The assessments must be based on factors that include but are not limited to the treatment needs of individual program participants, participants' with tendencies to victimize others, participants' vulnerability to being victimized, the unit's population mix, and the influence of new admissions. C. The license holder must develop a written plan that identifies specific participant characteristics related to resource utilization and specifies methods for evaluating the effectiveness and adequacy of staffing levels necessary to provide active treatment, support order, and provide safety and security to staff and participants. D. Assessments must be completed as often as necessary but no less than quarterly. E. A team representing different staffing needs within the facility must complete the assessments and report the resulting data to the facility administration. F. The administration must review and consider the reported data as part of the continuing process of monitoring established staffing levels and reestablishing staffing levels as necessary. The administration must document when staffing changes are made due to assessment data. G. The license holder must develop policies and procedures for implenting the requirements of this subpart. |
Variance #8 to Minnesota Rules, part 9515.3050, subpart 3, item B. A. The assessment performed by the license holder to determine the appropriateness of staffing levels at a minimum must include the following factors:
B. The written plan required of the license holder may be included in the policies and procedures, provided the plan otherwise meets the requirements of this subpart. |
| 9515.3060 STAFF QUALIFICATIONS. Subpart 1. Program director. The program director must have at least one year of work experience or training in administration or supervision, plus: A. at least a master's degree in the behavioral sciences or related field plus at least two years of work experience providing services to sex offenders or to persons with behavioral disorders, developmental disabilities, mental illness, or chemical dependency; or 8. a bachelor's degree in the behavioral sciences or related field from an accredited college or university plus a minimum of four years of work experience providing services to sex offenders or to persons with behavioral disorders, developmental disabilities, mental illness, or chemical dependency. |
|
| Subp. 2. Treatment staff and treatment support staff qualifications. A. Treatment staff members and consultants whose duties require them to be licensed, certified, or registered by the state of Minnesota must have a copy of their current license, certification, or registration in their personnel files. B. Treatment staff members who provide assessments and individual and group counseling services must be qualified in at least one of the following ways: (1) have a bachelor's degree in one of the behavioral sciences or related fields from an accredited college or university and at least 2,000 hours of supervised experience providing services to sex offenders or to persons with behavioral disorders, developmental disabilities, mental illness, or chemical dependency; (2) have at least 6,000 hours of supervised experience in providing services to sex offenders or to persons with behavioral disorders, developmental disabilities, mental illness, or chemical dependency; (3) be a graduate student in one of the behavioral sciences or related fields and be formally assigned by an accredited college or university to the facility for clinical training under the supervision of a qualified treatment staff member or consultant; or (4) hold a master's or other graduate degree from an accredited college or university in one of the behavioral sciences or related fields. C. A treatment staff member who provides services and programming to implement participant treatment plan objectives such as completing educational and vocational goals, identifying appropriate recreation and leisure activities, and developing social relationships with peers must, at a minimum: (1) have completed at least two years of post-secondary education at an accredited college or university with a minimum of 18 quarter hours or 12 semester hours in the behavioral sciences, social work, or nursing; or (2) have been employed at least 2,000 hours providing direct services to: sex offenders or to persons with behavioral disorders, mental illness, developmental disabilities, or chemical dependency. D. Treatment support staff must be at least 18 years old and have a high school diploma or a general education degree (GED). |
|
| 9515.3070 STAFF ORIENTATION AND DEVELOPMENT. Subpart 1. Initial staff orientation and training. The license holder is responsible for ensuring that every staff member successfully completes the orientation training specified in items A and B. A. Before providing direct care or having any other direct contact with persons in treatment, a staff member must: (1) complete an overview of the treatment program philosophy and design; (2) demonstrate mastery of techniques used to manage behavioral emergencies, including preventive de-escalation techniques and physical and nonphysical intervention techniques to interrupt violent behavior; (3} be knowledgeable about the rights of persons in treatment under applicable laws such as Minnesota Statutes, sections 144.651 (the Patient Bill of Rights) and 626.557 (the Reporting of Maltreatment of Vulnerable Adults Act), and about program policies ensuring these rights. (4) understand how the general need to establish and maintain boundaries in a therapeutic relationship applies in the specific context of working with sexual psychopathic personalities and other sex offenders; and (5) review the program's emergency provisions on fire, weather, missing persons, serious injury, and death. B. With in the first 30 caleJldar days of employment. al I staff members must complete introductory training in: (1) human sexuality and specific issues raised by the program population; (2) awareness of the influences of culture and the importance of cultural differences; (3) control of infection and infectious diseases; and (4) assessment and individual treatment planning. |
|
| Subp. 2. Ongoing individual staff development and evaluation plan. The license holder must ensure that an individual staff development and evaluation plan is developed and implemented for all staff who provide, supervise, or administer direct services. The plan must: A. be developed within 90 days of employment and be reviewed and revised at least annually; B. meet the staff development needs specified in the staff member's annual employee evaluation; and C. address the specific age. cultural, and mental health needs of the persons being served. |
Variance #9 to Minnesota Rules, part 9515.3070, subpart 2. item A. A. The license holder must maintain an overall staff development and evaluation plan for all staff employed by MSOP. The plan must be documented and must address the specific age, cultural, and mental health needs of the clients being served. The staff development plan must be reviewed and revised annually. B. A performance review of each staff person must be conducted annually and must include an evaluation of the training completed by the individual staff person in the last 12 months and must identify the future training needs of that staff person. C. Documentation of training completed by staff must be maintained. |
| Subp. 3. Amount of annual training. The license holder must ensure that all staff receive the amount of training specified in this subpart. A. Except as provided in items B and C, all staff must receive at least 16 hours of training annually. B. Staff who work more than halftime and have less than 4,000 hours of experience providing services to sex offenders or to persons with behavioral disorders, developmental disabilities, mental illness, or chemical dependency must receive at least 24 hours of training annually. C. Treatment staff members and consultants whose duties require them to be licensed, certified. or registered by the state of Minnesota are exempt from the requirements in items A and B as long as they meet the training requirements necessary to remain current in their licensure, certification, or registration. The orientation required in subpart 1 may be counted toward the annual training requirement in an employee's first year of service. |
|
| Subp. 4. Content of training. The license holder must ensure that at least 75 percent of the required training hours is focused on one or more of the following areas or subjects: A. use of preventive de-escalation techniques and physical and nonphysical intervention to interrupt violent behavior; B. application and compliance with Minnesota Statutes and rules related to treatment and services for sex offenders; C. assessment and treatment of persons with special needs related to conditions such as substance abuse, obsessive compulsive disorder, organic brain damage, impulse control disorders, or other physical needs; D. prevention and control of infectious diseases, including human immunodeficiency virus (HIV) infection; E. how to administer first aid and cardiopulmonary resuscitation (CPR); and F. review of research, practice, or regulations that affect care and treatment programs for sex offenders. |
|
|
9515.3080 PROGRAM SAFETY AND RULES FOR BEHAVIOR. Subpart l. Program safety. The license holder must develop and follow policies and procedures for maintaining a secure and orderly environment that is safe for persons in treatment and staff and supportive of the treatment program. |
|
| Subp. 2. Written rules for behavior and consequences of violations. The license holder must specify rules of behavior for persons in treatment that are consistent with maintaining program safety and supportive of the person's rights to treatment. The rules must be in writing and must include a range of consequences that may be imposed for violation of the rules. The license holder must review and approve the written rules and range of consequences at least annually. The license holder must give each person in treatment a copy of the rules and consequences in a handbook or comparable format at the time of admission. If a person is unable to understand the written rules and consequences, the license holder must make the rules and consequences available in a form that the person can understand. The license holder must also give each staff member a copy of the written rules and consequences and ensure that the contents are discussed in the orientation required by part 9515.3070. |
|
| Subp. 3. Criteria for written rules. The written rules and consequences in subpart 2 must: A. regulate only behavior that endangers persons in treatment or others or threatens the license holder's ability to maintain the order and safety of the treatment program; and B. be clearly and objectively stated in terms of observable behavior. |
|
| 9515.3090 BEHAVIOR MANAGEMENT AND PROGRAM
SAFETY. Subpart 1. Behavior management. Disciplinary restrictions, emergency seclusion, and protective isolation may be imposed in accordance with this part when necessary to ensure a safe, secure, and orderly environment for the treatment program. For purposes of this part, disciplinary restrictions, emergency seclusion, and protective isolation have the meanings in subparts 2 to 4. |
Clarifications A. Clients may only be placed or remain in a room from which they are not able or permitted to exit when:
C. The Licensing Division will evaluate the license holder's compliance with all policies and procedures that apply to the program, including those related to administrative restriction under Minnesota Rules, part 9515.3040, subpart 2, item E. |
| Subp. 2. Disciplinary restrictions. "Disciplinary restrictions" means withholding or limiting privileges otherwise available to a person in treatment as a consequence of the person's violating rules of behavior. Examples of disciplinary restrictions would include withholding or limiting such privileges as work, leisure, vocational and recreational activities. or access to parts of the facility. Disciplinary restrictions must: A. be in proportion to the rule's importance to the order, safety, and security of the treatment program and to the severity of the violation; B. be reasonably related to the nature of the behavior; and C. take into consideration the person's past behavior while in the program. |
|
|
"Emergency seclusion" means an emergency intervention that physically separates the person in treatment from others, including placing the person in a room from which the person is not able or permitted to exit.
Emergency seclusion does not include locking a person in the person's sleeping room during normal sleeping hours or limiting a person's access to parts of the facility to which the person would otherwise have access. Emergency seclusion must be: A. imposed only when necessary to protect the person being secluded or another person or individual from imminent danger of serious physical harm or to prevent serious property damage. B. Authorized by the nurse on duty who must immediately contact a physician for an order; and C. continued only as long as the person's behavior indicates imminent danger continues. Staff must monitor the person in emergency seclusion no less than every 15 minutes. Every physician must review the situation at least every 24 hours. |
Variance #10 to Minnesota Rules, part 9515.3090, subpart 3, including items Band C. A. Observation status is used when it is determined that a client whose clinical or medical status requires additional supervision, observation, or restricted access to items the client could use to harm him- or her- self. Observation status may include physically separating the client from others. When the separation occurs in a room from which the client is not able or permitted to exit, it is considered seclusion and subject to the requirements of Minnesota Rules, part 9515.3090, subpart 3. Clients placed in seclusion shall be moved to the high security area of the facility. B. Prior to placing a client in seclusion, it must be determined that this level of intervention is necessary due to the client being in imminent danger of serious physical harm to him- or her-self. Seclusion may occur over normal sleeping hours and may limit the client's access to the facility. C. During regular business hours, the use of seclusion shall only be authorized by a medical practitioner, licensed psychologist, license-eligible psychologist, or clinical director of the program who meets with the client to determine what level of observation is required, if any. During non-business hours, including weekends, holidays, evenings and sleeping hours, the use of seclusion shall be authorized by a licensed health services staff whom conducts an assessment of the client and consults with the medical practitioner who is on-call. D. Staff must check the client in seclusion in person at least every 15 minutes or continuously monitor the client. The level of monitoring that is required to assure the client's safety is determined by the medical practitioner, licensed psychologist, license-eligible psychologist, or clinical director. E. After the first 24-hour period of the client being placed in seclusion, the clinical director, a licensed psychologist, license-eligible psychologist, or a medical practitioner must reassess the client's need for seclusion and may renew or terminate the use of seclusion. The action must be documented in the client's file. If the 24 hour period occurs on a weekend, holiday, or during the evening or overnight shift the medical practitioner who is on-call shall review the placement and determine whether to renew or terminate the use of seclusion. This action must be documented in the client's file. F. Staff must document in the client record the use of seclusion, the reason it was implemented, who authorized it, and each review including the name of the treatment staff member who assessed whether it was necessary to continue or terminate. G. MSOP must have a policy and procedure to address situations in which the license holder has determined that emergency seclusion is to be discontinued and the client refuses to leave the high security area. The policy and procedures must include what steps the license holder will take to transition the client from the high security area. |
| Subp. 4. Protective isolation. ~Protective isolation" means placing a person in treatment in a room from which the person is not able or permitted to exit as a way of defusing or containing dangerous behavior that is uncontrollable by any other means. The license holder must have written policies on protective isolation that cover the points in items A to C. A. Protective isolation must not be used for the convenience of staff or as a substitute for programming. B. Treatment must be available during protective isolation to the extent that the person's behavior and condition make treatment possible; treatment shall include components designed to eliminate or reduce the specified behavior or behaviors that caused the need for protective isolation. C. Protective isolation must not go beyond 48 continuous hours unless the treatment team recommends continuation to the medical director in a statement that:
|
Variance #11 to Minnesota Rules, part 9515.3090, subpart 4, item C. A. Protective isolation {Pl) status means placing a client in a room from which the client is not able or permitted to exit, as a way of defusing or containing dangerous behavior that is uncontrollable by any other means. At the facility in Moose Lake, this may only occur in the high security area unless there is a specific documented need for Pl to occur outside of the high security area. Clients who are placed NOTE: MSOP's policy defines dangerous behavior as "behavior that compromises the safety or security of the treatment program, or disrupts the order of the program to the extent that safety or security may be jeopardized." B. The following three conditions must be met before protective isolation is used:
C. Immediately following a client being placed on protective isolation status, the Officer of the Day must be notified. The Officer of the Day must assess whether the criteria identified in Minnesota Rules, part 95 I 5.3090. subpart 4 (i.e. paragraph B of this section, conditions 1 through 3) were met based on the information that is available. If they were not met, the client must be released from protective isolation status immediately. Within four hours of a client being placed on protective isolation status, the Officer of the Day must review the initial decision based on any additional information that has become available to evaluate whether the criteria defined in Minnesota Rules, part 9515.3090, subpart 4 {i.e. paragraph B of this section, conditions 1 through 3} are met based on the competed documentation of all staff, including all related incident reports. If the criteria are not met. the client must be released from protective isolation status immediately. D. The client must be monitored every 15 minutes or at a frequency established by the Officer of the Day. If the Officer of the Day establishes a frequency of monitoring that is more or less than 15 minutes, it must be documented. Each occurrence of monitoring of the client by staff must be documented. E. The Officer of the Day must assure the documentation identifying why the protective isolation was initiated and what less restrictive means were attempted to manage the behavior is complete. F. At 24 hours of a client being placed in protective isolation and within every 24 hours thereafter (until the client is discharged from protective isolation), the Officer of the Day must assess whether the criteria defined in Minnesota Rules, part 9515.3090, subpart 4 (i.e., paragraph B of this section. conditions 1 through 3), were met based on the completed documentation of staff, including all related incident reports. If the criteria are not met, the client must be released from protective isolation immediately. The Officer of the Day must document this assessment was completed. G. The assessment that occurs every 24 hours must also evaluate whether the client is being provided programming designed to eliminate or reduce the specified behavior or behaviors that caused the need for protective isolation. The license holder is responsible to assure that this programming is provided. H. ln order for protective isolation to continue beyond 48 hours, the treatment team must recommend its continuation. In cases where the treatment team recommends continuation of protective isolation, the recommendation must be in writing and meet the requirements of Minnesota Rules, part 9515.3090, subpart 4, paragraph C, items ( I ) through ( 8). In cases where the treatment team recommends that protective isolation be discontinued, but the client refuses to leave protective isolation, the staff must document every 48 hour period what attempts were made to have the client leave protective isolation. Every 48 hours this documentation must be reviewed by the Medical Director or his or her designee. NOTE: If a client no longer meets the conditions to remain in protective isolation status, but refuses to leave the high security area, the client's ITP must include steps to transition the client from the high security area. I. In lieu of the Medical Director, MSOP may designate staff to evaluate whether the recommendation for continuing the use of protective isolation beyond 48 hours may be approved. The evaluation must consider all of the information and data required under Minnesota Rules, part 9515.3090, subpart 4, paragraph C, items (I) through (8). When the review is conducted by a designee of the Medical Director, the designee must assess and document whether the use of the protective isolation complies with Minnesota Rules. part 9515.3090, subpart 4, including conditions l through 3 in paragraph B of this section. If approved, the approval must be documented in the client's record. J. The following individuals may act as designees to the Medical Director for purposes of this subpart.
L. If it is determined by the Licensing Division that the review completed by a designee of the Medical Director did not comply with Minnesota Rules, part 9515.3090 the Licensing Division may rescind that individual's authority to approve such recommendations. M. Each week the program's Protective Isolation Review Panel shall review the documentation concerning clients who have been placed in protective isolation or remain in protective isolation since the last weekly review. The program's Protective Isolation Review Panel shall discontinue protective isolation if the documentation does not provide evidence that the criteria required under Minnesota Rules, part 9515.3090, subpart 4 to initiate or continue protective isolation was met. N. The license holder must clearly document when protective isolation is discontinued, but the placement in the high security area is continued. O. MSOP must have a policy and procedure to address situations in which the license holder has determined that protective isolation is to be discontinued and the client refuses to leave the high security area. The policy and procedures must include what steps the license holder will take to transition the client from the high security area. |
| Subp. 5. Request for review of protective isolation. The license holder must provide to a person in treatment who is placed in protective isolation a procedure which can be used immediately to request a review if the person believes the placement was unwarranted. Protective isolation may be imposed pending the outcome of the review. The review request procedure must include the elements in items A to D. A. The review must be conducted by a panel of at least three persons, who were not participants in the decision to impose the isolation, and whose professional experience and training qualify them to assess the situation. B. The review must be conducted and the outcome determined within seven days of being requested, excluding Saturdays, Sundays, and legal holidays, unless the review panel states in writing why a determination cannot be made within seven days and specifies when a determination will be made. C. The person requesting the review must have the opportunity to present to the review panel evidence and argument to explain why protective isolation is unwarranted. The review panel may reasonably limit the form by which the evidence and argument are presented if necessary to ensure the physical safety of he review participants. D. A person may request that the chief officer of the facility review a determination of the review panel. The chief officer's decision is final. |
Variance #12 to Minnesota Rules, part 9515.3090, subpart 5, item D. A. A client who is placed in protective isolation may request a review by the Protective Isolation Review Panel if the client believes the placement was not warranted. The review panel must review the client's placement on a weekly basis as long as a client remains in protective isolation. These reviews occur regardless of the client's request. The review will include whether protective isolation will be continued or be terminated. If is continued, the pane I will determine whether the protective isolation plan will be modified. 8. The client must have the opportunity to present evidence to the review panel and to explain why he or she believes that the placement in protective isolation is unwarranted. The review panel may reasonably limit the forum by which the evidence is presented if necessary to ensure the physical safety of the review participants. C. The review of the use of protective isolation must be conducted and the outcome determined within seven days of protective isolation being initiated, excluding Saturdays, Sundays, and legal holidays, unless the review panel states in writing why a determination cannot be made within seven days and specifies when a determination will be made. The determination made by the protective isolation review panel must be documented on the protective isolation review form and maintained in the client record. D. MSOP may designate the Moose Lake Facility Director to review and make a final decision of any appeals to the determination of the Protective Isolation Review Panel at Moose Lake. E. MSOP may designate the St. Peter Facility Director to review and make a final decision of any appeals to the determination of the Protective Isolation Review Panel at St. Peter. F. MSOP will maintain a separate appendix on file with the Licensing Division specifying the current names of individuals assigned to positions identified in items D and E who are designated to make final determinations concerning appeals of the use of protective isolation, under this section. G. MSOP must have a policy and procedure. including related forms for the use of protective isolation. The policy and procedure must comply with Rule 26 and this variance and be dated. The forms must clearly document the reason protective isolation was initiated, what less restrictive actions were attempted by staff to address the situation, and a summary of the incident reports that lead to protective isolation being required. The policy and procedure must be approved by the MSOP Executive Director or designee. |
| 9515.3100 ADMINISTRATIVE RECORDS. Subpart 1. Staff records. The license holder must maintain personnel records on all staff. The staff records must include the following information: A. documentation that a background study has been done as required by Minnesota Statutes, section 245A.04, subdivision 3; B. documentation of a staff person's education and experience, including current licensure, certification. or registration when require by a person's position; and C. documentation of staff orientation and training. The record must include the date orientation or training was completed, the topics covered, and the hours of training received. |
|
| Subp. 2. General administrative records. The license holder must maintain the following administrative records and make the records available to the commissioner for inspection: A. a directory of all persons in the treatment program; B. a copy of the facility's licenses from the commissioner and the commissioner of health; C. a copy of the purchase of service contracts and subcontracts with a consultant and other individuals who provide services in the residential program, but who are not under the direct control of the license holder; and D. a copy of the facility's quality improvement plan, including reports that monitor and evaluate current activities. |
|
| 9515.3110 RECORDS OF PERSONS IN TREATMENT. Subpart 1. Central record file on premises. The license holder must maintain a central file of persons' records on the program premises. |
Variance #13 to Minnesota Rules, part 9515.3110, subpart 1. A. All treatment records of current clients for the preceding 12 month period must be maintained on-site and must be readily accessible and continuously available to authorized MSOP personnel. B. All clinical records and chart notes must be maintained in the client record and must be available in the client record within seven (7) calendar days of completion. C. All treatment records stored in an off-site location must be stored in the same area of a leased building. D. All records must be protected from loss. tampering. defacement, or use by unauthorized persons and must be maintained and used in accordance with all applicable regulations governing data practices. E. All records stored off-site must be secured and readily accessible and continuously available to authorized MSOP personnel. |
| Subp. 2. Admission record. Each person's admission record must include: A. the person's name, date of birth, and social security number; B. a photograph taken at admission; C. the date of admission; D. the name, address, and telephone number of an individual tocontact in case of an emergency; E. documentation that the person's legal or medical status meets admission criteria; F. names of victims identified as requiring or requesting protection from the person or notification of the person's release or change of status; and G. names and telephone numbers of the person's attorney, county case manager, and any other individual warranted by the person's legal or medical status. |
Variance #14 to Minnesota Rules, part 9515.3110, subpart 2, items A and F. A. The client's social security numbers will be collected and available to those with security access, but will not be included in the client's record. B. The names of victims identified as requiring or requesting protection from the client or notification of the client's release or change of status will not be place in the client record but will be maintained in a secure administrative file. |
| Subp. 3. Treatment records. The license holder must document the course of evaluation and treatment for each person in treatment. In addition to any other documentation the license holder chooses to include, each person's record must contain: A. copies of the person's diagnostic assessment, individual treatment plan, progress notes, quarterly evaluation, and discharge plan; B. names of the person's medical providers; C. documentation of incidents or emergencies involving the person; D. copies of any State Review Board reports on the person; and E. a copy of the person's transfer and discharge summary when applicable. |
|
| Subp. 4. Consent to release information in record. The license holder shall not release information in a person's record without a written consent signed by the person that specifies: A. the date of authorization and length of time, not to exceed 6 months from the date of the person's signature, for which the consent is valid; B. the information that will be released; C. the purpose for releasing the information; and D. the name of the individual or organization authorized to receive the information. |
Variance #15 to Minnesota Rules, part 9515.3110, subpart 4, item A. A. The client's consent to authorize the release of information is in writing and maintained in the client's record. B. The consent to release information shall be valid for no more than 365 calendar days from the date of signature and must comply with Minnesota Statutes, section 13.05 subdivision 4, paragraph (d). |
| Subp. S. Secure confidential file. Confidential information that is not to be released to a person must be kept separate from the person's medical record in a secure confidential file. The file must be accessible to staff 24 hours a day. |
Exhibit G: Minn. Stat.§ 253B.02 Subd. 13 (a). Person who is mentally ill.
(a) A person who is mentally ill means any person who has an organic disorder of the brain or a substantial psychiatric disorder of thought, mood, perception, orientation, or memory which grossly impairs judgment, behavior, capacity to recognize reality, or to reason or understand, which is manifested by instances of grossly disturbed behavior or faulty perceptions and poses a substantial likelihood of physical harm to self or others as demonstrated by:
- a failure to obtain necessary food, clothing, shelter, or medical care as a result of the impairment;
- an inability for reasons other than indigence to obtain necessary food, clothing, shelter, or medical care as a result of the impairment and it is more probable than not that the person will suffer substantial harm, significant psychiatric deterioration or debilitation, or serious illness, unless appropriate treatment and services are provided;
- a recent attempt or threat to physically harm self or others; or
- recent and volitional conduct involving significant damage to substantial property.
(b) A person is not mentally ill under this section if the impairment is solely due to:
- epilepsy;
- developmental disability;
- brief periods of intoxication caused by alcohol, drugs, or other mind-altering substances; or
- dependence upon or addiction to any alcohol, drugs, or other mind-altering substances.
Exhibit H: DSM 2nd Paragraph
Use of the manual
Individuals with the disorder who share certain features (e.g., major depressive disorder, with mixed features) and to convey information that is relevant to the management of the individual's disorder, such as the "with other medical comorbidity" specifier in sleep-wake disorders. Although a fifth digit is sometimes assigned to code a subtype or specifier (e.g., 294.11 (F02.81] major neurocognitive disorder due to Alzheimer's disease, with behavioral disturbance) or severity (296.21 [F32.0] major depressive disorder, single episode, mild), the majority of subtypes and specifiers included in DSM-5 cannot be coded within the ICD-9-CM and ICD-10-CM systems and are indicated only by including the subtype or specifier after the name of the disorder (e.g., social anxiety disorder [social phobia], performance type). Note that in some cases, a specifier or subtype is codable in ICD-10-CM but not in ICD-9-CM. Accordingly, in some cases the 4th or 5th character codes for the subtypes or specifiers are provided only for the ICD-10-CM coding designations.
A DSM-5 diagnosis is usually applied to the individual's current presentation; previous diagnoses from which the individual has recovered should be dearly noted as such. Specifiers indicating course (e.g., in partial remission, in full remission) may be listed after the diagnosis and are indicated in a number of criteria sets. Where available, severity specifiers are provided to guide clinicians in rating the intensity, frequency, duration, symptom count, or other severity indicator of a disorder. Severity specifiers are indicated by the instruction "Specify current severity" in the criteria set and include disorder-specific definitions. Descriptive features specifiers have also been provided in the criteria set and convey additional information that can inform treatment planning (e.g., obsessive-compulsive disorder, with poor insight). Not all disorders include course, severity, and/ or descriptive features specifiers.
Medication-Induced Movement Disorders and Other Conditions That May Be a Focus of Clinical Attention
In addition to important psychosocial and environmental factors (see "The Multiaxial System" in the "Introduction" elsewhere in this manual), these chapters in Section II also contain other conditions that are not mental disorders but may be encountered by mental health clinicians. These conditions may be listed as a reason for clinical visit in addition to, or in place of, the mental disorders listed in Section II. A separate chapter is devoted to medication-induced disorders and other adverse effects of medication that may be assessed and treated by clinicians in mental health practice such as akathisia, tardive dyskinesia, and dystonia. The description of neuroleptic malignant syndrome is expanded from that provided in DSM-IV-TR to highlight the emergent and potentially life-threatening nature of this condition, and a new entry on antidepressant discontinuation syndrome is provided. An additional chapter discusses other conditions that may be a focus of clinical attention. These include relational problems, problems related to abuse and neglect, problems with adherence to treatment regimens, obesity, antisocial behavior, and malingering.
Principal Diagnosis
When more than one diagnosis for an individual is given in an inpatient setting, the principal diagnosis is the condition established after study to be chiefly responsible for occasioning the admission of the individual. When more than one diagnosis is given for an individual in an outpatient setting, the reason for visit is the condition that is chiefly responsible for the ambulatory care medical services received during the visit. In most cases,
the principal diagnosis or the reason for visit is also the main focus of attention or treatment. It is often difficult (and somewhat arbitrary) to determine which diagnosis is the principal diagnosis or the reason for visit, especially when, for example, a substance-related diagnosis such as alcohol use disorder is accompanied by a non-substance-related
diagnosis such as schizophrenia. For example, it may be unclear which diagnosis should
Exhibit I: Minn. Stat. § 253D.07 Subd. 3M
Subdivision 1. Before commitment proceedings are instituted, the facts shall first be submitted to the county attorney, who, if satisfied that good cause exists, will prepare the petition. The county attorney may request a prepetition screening report. The petition is to be executed by a person having knowledge of the facts and filed with the district court of the county of financial responsibility, as defined in section 253B.02, subdivision 4c, or the county where the respondent is present. If the respondent is in the custody of the commissioner of corrections, the petition may be filed in the county where the conviction for which the person is incarcerated was entered.
Subd. 2. Upon the filing of a petition alleging that a proposed respondent is a sexually dangerous person or a person with a sexual psychopathic personality, the court shall hear the petition as provided in sections 253B.07 and 253B.08.
Subd. 3. If the court finds by clear and convincing evidence that the respondent is a sexually dangerous person or a person with a sexual psychopathic personality, the court shall commit the person to a secure treatment facility unless the person establishes by clear and convincing evidence that a less restrictive treatment program is available, is willing to accept the respondent under commitment, and is consistent with the persons treatment needs and the requirements of public safety.
Subd. 4. After a determination that a respondent is a sexually dangerous person or a person with a sexual psychopathic personality, the court shall order commitment for an indeterminate period of time and the committed person shall be transferred, provisionally discharged, or discharged, only as provided in this chapter.
Subd. 5. Not to constitute defense. The existence in any person of a condition of a sexual psychopathic personality or the fact that a person is a sexually dangerous person shall not in any case constitute a defense to a charge of crime, nor relieve such person from liability to be tried upon a criminal charge.